
























– Removed consideration for prior COVID-19 vaccination or booster status for determination of isolation, quarantine, or indications for testing.
– Increased testing frequency after exposure to three tests within 7 days.
– Changed the length of isolation for COVID-19 patients with moderate illness to 10 days.
– Changed the length of isolation for COVID-19 patients with severe to critical illness to at least 10, and up to 20 days, depending on resolution of symptoms including fever and repeat negative test results. Definition of severe-critical illness are included below.
– Updated re-testing recommendations after initial COVID-19 diagnosis to begin consideration for re-testing with symptoms or new exposure after 30 days from initial diagnosis.
The updated guidance is published in the IP Clinical Library.
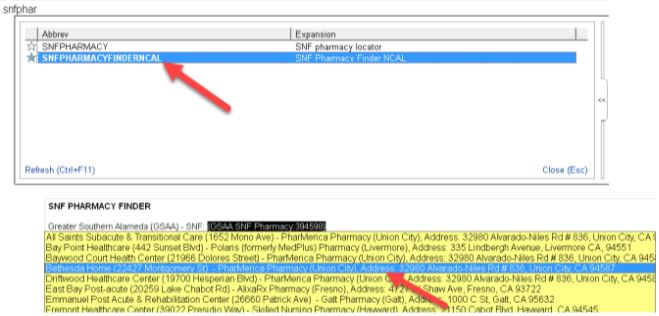
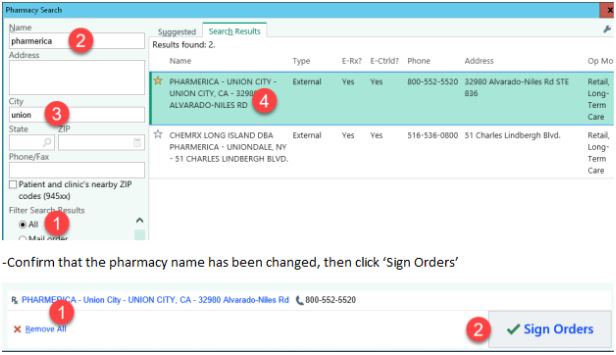
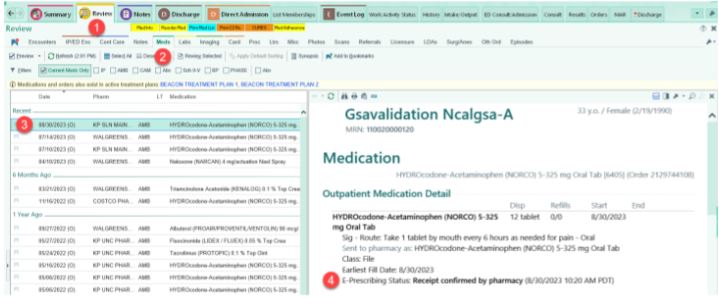
Workflow for Sure Scripts
Just a reminder that with the Fall Upgrade on 9/23, the LETTERS ACTIVITY is no longer be available. To complete patient letters, everyone will use Communications instead.
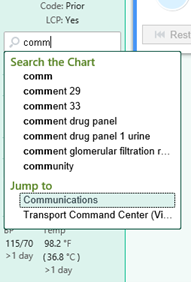
How do I get to Communications?
You can use Chart Search to access it. Type ‘Comm’ in search bar on left side and select ‘Communications’
How do I use Communications?
Select ‘New Communication’
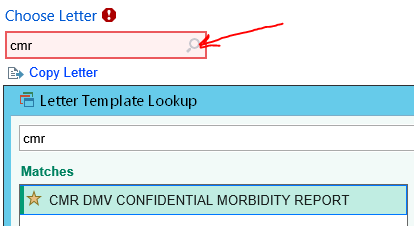
Enter ‘CMR’ in Choose Letter section, click the magnifying glass to search, and then select ‘CMR DMV CONFIDENTIAL MORBIDTY REPORT’
Click on ‘Details’ to see Reason for Letter, which should be set automatically to ‘CMR – Not online’ . This option ensures that the letter will NOT be sent/available online in patient’s KP.org account.

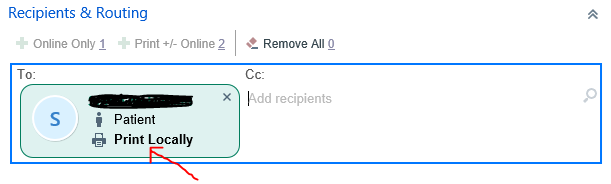
Select ‘Print +/-Online’ in the Recipient & Routing section. You will see the patient’s name in the ‘To:’ field with ‘Print Locally’ option. This just means that the letter will be printed locally, will NOT be sent to patient.
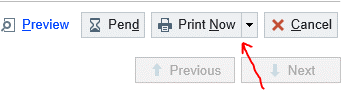
Select ‘Print Now’ option on the right lower corner and select the local printer to print the letter
KPHC Full Outage – Saturday, September 23, 2023, 1:00 AM – 2:30 AM. Please use down time forms during this time.
Just a reminder that the kick off is coming 8/21/23
No new information since the presentation by James last month.
In brief:
Please use CHF orderset.
Please use CHF DC specific drop down menu in summary.
CHF DCI still not available as of today per region. Will update once it is available. Please use current .DCU with current drop down CHF instruction as appropriate.
Come have an amazing time in the sun with your colleagues and their family / pets! We will have tacos / quesadillas (grilled on site) along with an assortment of beverages (both alcoholic and non-alcoholic) and snacks! Lots of fun activities for the kids as well! We have reserved the picnic tables under the Pavilion. There is a big playground at this park catered to both young and older children.
When: Saturday September 16, 2023 from 1 – 5pm
Where: Jean Sweeney Open Space Park. 1100 Atlantic Ave, Alameda, CA 94501
Who: You + Immediate family + Pets
What to bring: Picnic Blankets, Sunscreen
Sponsored by : PHW & PICs
Departments: HBS, Cardiology, Urology, Infectious Disease, Interventional Radiology, Gastroenterology, Special Guests : Eric & Kapil
Questions?: Email Jeannie at hoa.n.tran@kp.org or text 510-203-2949
Powered by WordPress & Theme by Anders Norén